Nutrient Absorption in the Small Intestine
Pre-work
Medical Biochemistry, Chapter 30, 455-469
Lesson
Click the slide below to start the presentation:
Review of Primary Locations for Nutrient Absorption
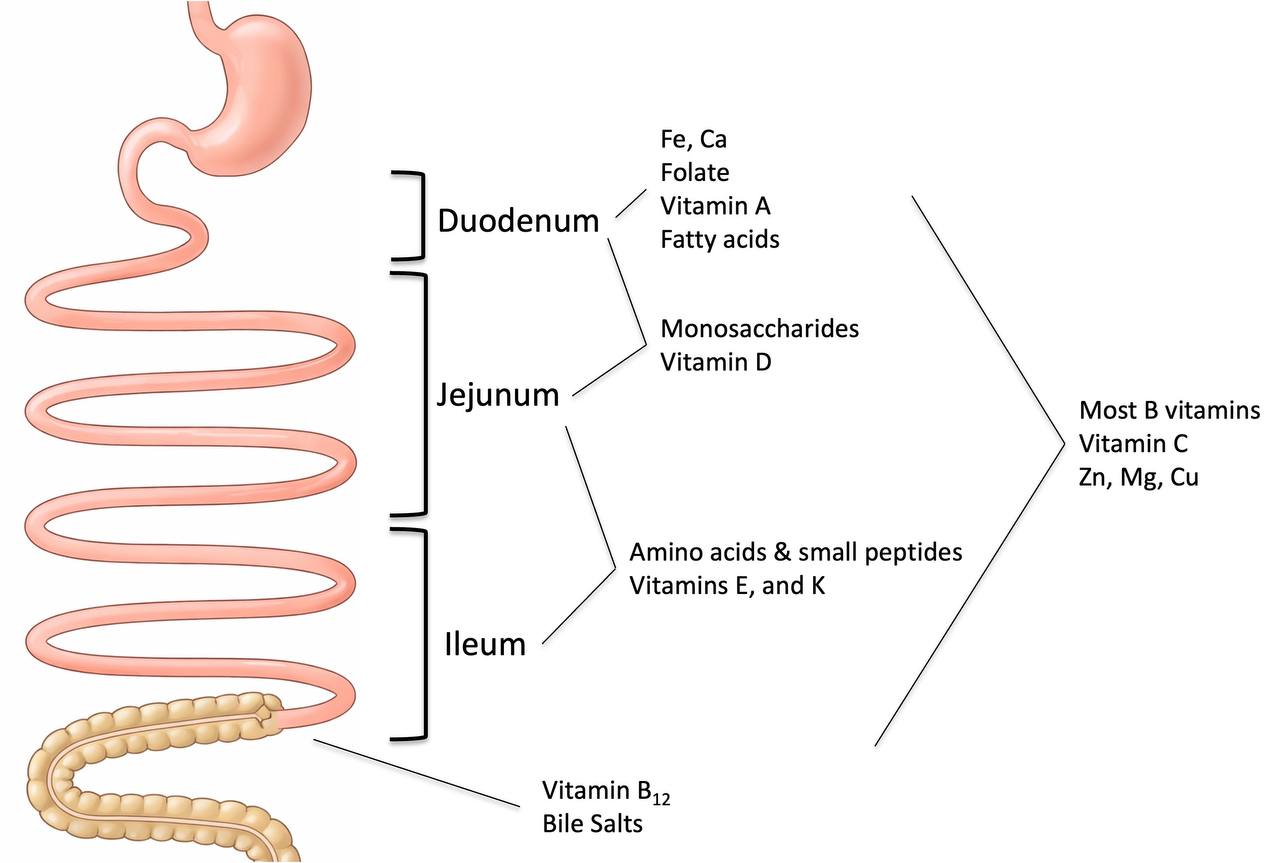
Image adapted from Pawlowski et al (2009) Gastroenterology 136: 1874-86
Clinical Case
A 41-year-old woman of Algerian descent, referred by her gynecologist, presented with a blood hemoglobin of 7.8 g/dL. She was on hormone therapy for endometriosis and had essentially no menstrual bleeding for the past 5 years. She followed no dietary restrictions. Her serum ferritin was unmeasurable.
The patient's only symptom was shortness of breath with exertion, and except for pallor, her examination results were normal. Iron repletion with daily ferrous sulfate supplements increased her blood hemoglobin to 12 g/dL in 1 year. She continued taking iron supplements.
Four years later, she fractured her wrist after a low-impact fall. A bone mineral density study (DEXA scan) revealed osteoporosis.
What is the most likely underlying cause of her signs and symptoms?

Gaps in Knowledge
Questions
Questions will appear here...
Answers
Answers will appear here...
A 41-year-old woman of Algerian descent, referred by her gynecologist, presented with a blood hemoglobin of 7.8 g/dL. She was on hormone therapy for endometriosis and had essentially no menstrual bleeding for the past 5 years. She followed no dietary restrictions. Her serum ferritin was unmeasurable.
The patient's only symptom was shortness of breath with exertion, and except for pallor, her examination results were normal. Iron repletion with daily ferrous sulfate supplements increased her blood hemoglobin to 12 g/dL in 1 year. She continued taking iron supplements.
Four years later, she fractured her wrist after a low-impact fall. A bone mineral density study (DEXA scan) revealed osteoporosis.
What is the most likely underlying cause of her signs and symptoms?
- Cation transporter deficiency
- Chronic hepatitis B infection
- Chronic small intestine bacteria overgrowth
- Celiac Disease
Clinical Case
A 41-year-old woman of Algerian descent, referred by her gynecologist, presented with a blood hemoglobin of 7.8 g/dL. She was on hormone therapy for endometriosis and had essentially no menstrual bleeding for the past 5 years. She followed no dietary restrictions. Her serum ferritin was unmeasurable.
The patient's only symptom was shortness of breath with exertion, and except for pallor, her examination results were normal. Iron repletion with daily ferrous sulfate supplements increased her blood hemoglobin to 12 g/dL in 1 year. She continued taking iron supplements.
Four years later, she fractured her wrist after a low-impact fall. A bone mineral density study (DEXA scan) revealed osteoporosis.
What is the most likely underlying cause of her signs and symptoms?
Case Review
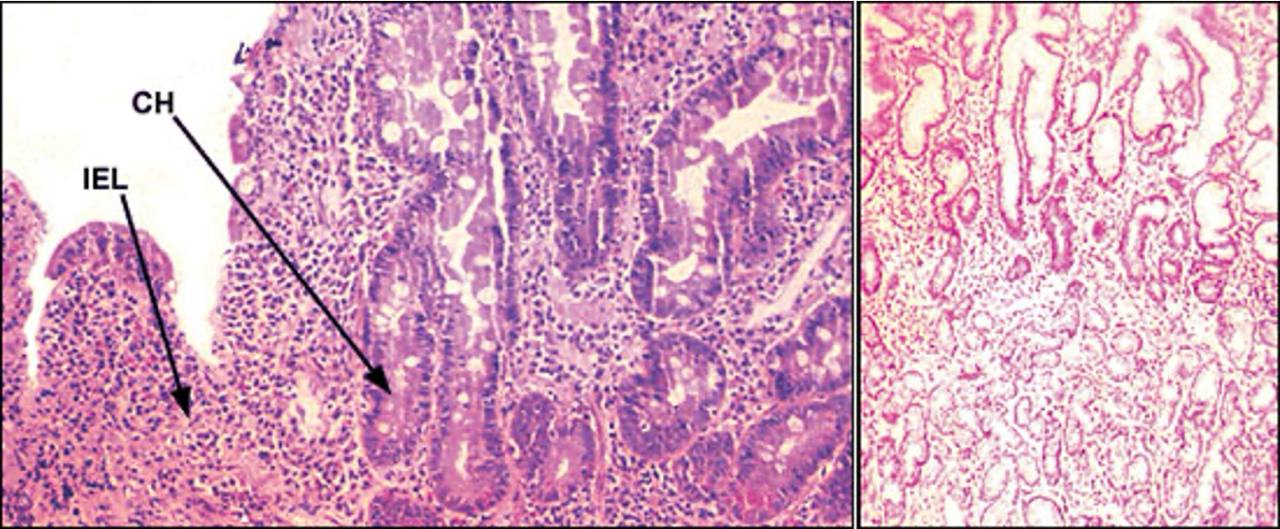
IEL = intraepithelial lymphocytes | CH = crypt hyperplasia | Source: Am Fam Physician. 2002 Dec 15;66(12):2259-2266.
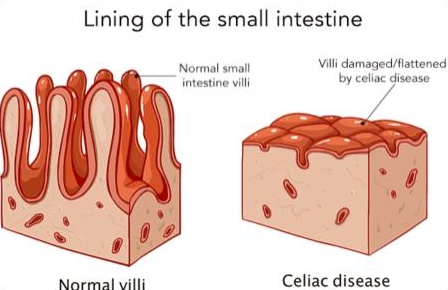
Why didn't she have any obvious GI symptoms?
Why not cation transporter deficiency?
- Iron and calcium use different transporters to cross cell membranes
- These transporters are separately regulated, and deficiency of either is rare
- Algerians have high rates of celiac disease in their population (~5%, source: JAMA. 2017;318(7):647-656.)
- Confirm celiac disease with tTG IgA antibody test while on gluten, followed by duodenal biopsy if positive
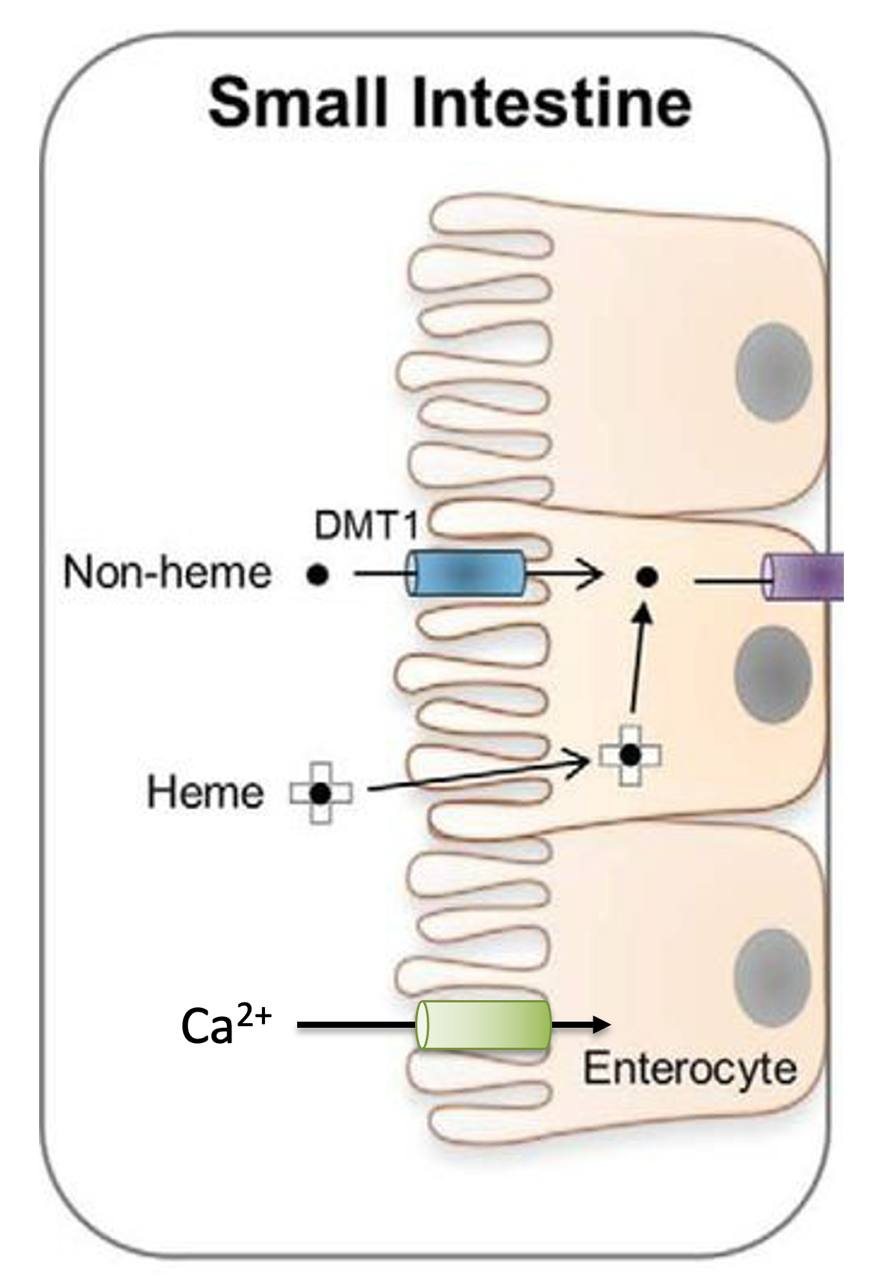
Image adapted from Knutson (2017) JBC 292(31):12735-12743